La pêche est associée à un sport et au plaisir de la chasse en mer. Elle peut se pratiquer de plusieurs façons : depuis la côte, en navigation avec votre bateau, mais également en plongée sous-marine en apnée, ...
C'est aussi le moyen de remplir le frigo ou le congélateur de votre bateau ou de votre maison. Voici quelques livres sur la pêche en mer pour vous aider, et pour les tourdumondistes vous pouvez également embarquer des livres de cuisine et idées de recettes à bord.
Nous vous conseillons également de consulter notre article consacré à l'avitaillement pour un tour du monde en voilier.
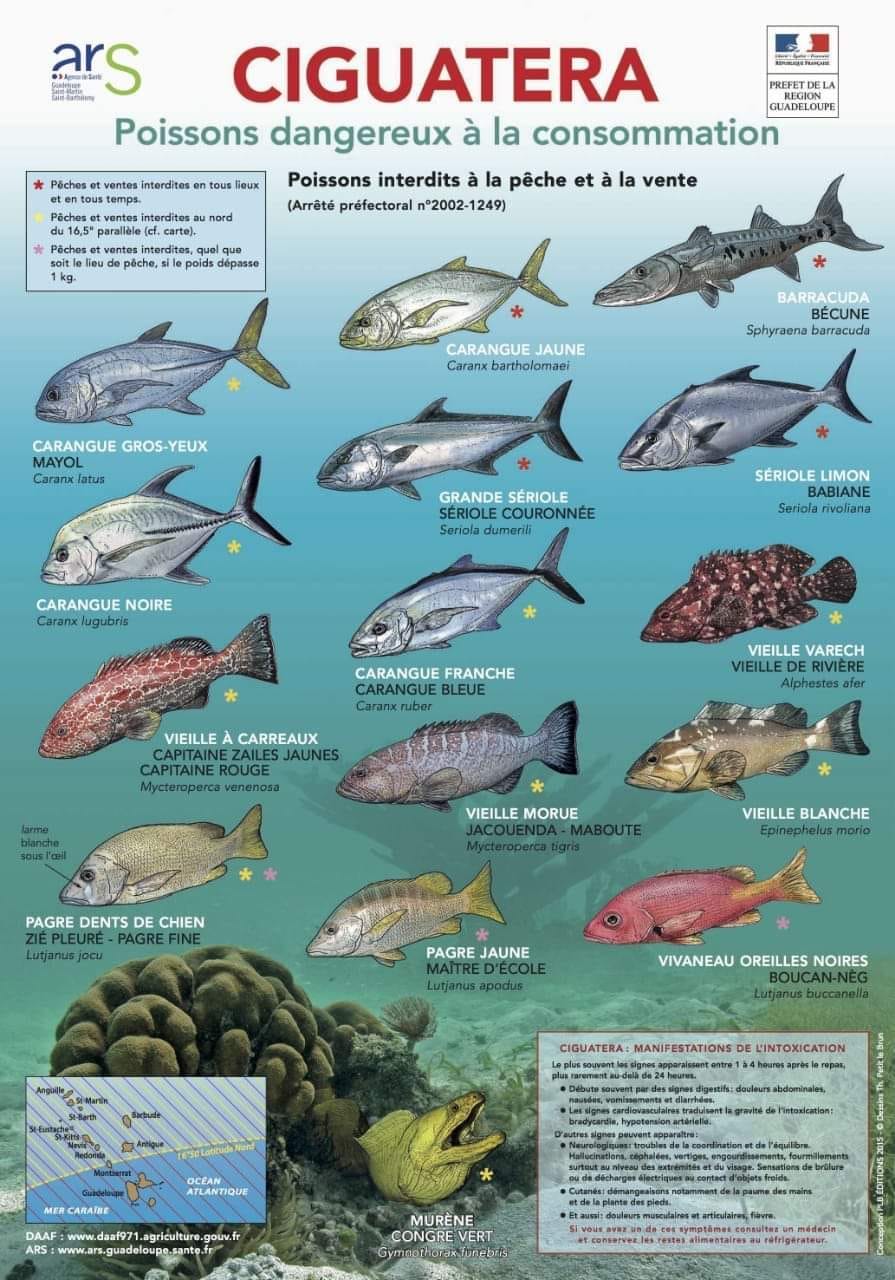
Mais attention, une bonne partie de pêche peut se terminer en une très grave intoxication : donc attention à la ciguatera ! Voici quelques livres pour identifier les poissons.
Remerciements à l'équipage de Sailing la Vagabonde pour cette vidéo.
La ciguatera ou icthyosarcotoxisme (du grec ichtyos : poisson, sarcos : chair, toxicon : toxique), ou "gratte" (appellation populaire en Nouvelle Calédonie) est une intoxication alimentaire liée à l'ingestion de poissons contaminés par la microalgue benthique Gambierdiscus toxicus présente dans les récifs coralliens.
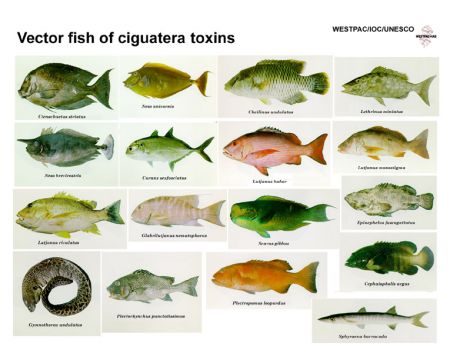
Comme de nombreuses toxines naturelles et artificielles, la ciguatoxine s'accumule dans les organismes et sa concentration augmente au fur et à mesure que l'on monte les échelons de la chaîne alimentaire, selon le principe de la biomagnification. Parmi les 400 espèces potentiellement infectées, les grands poissons prédateurs comme le barracuda, la murène, le mérou ou encore les carangues sont les plus susceptibles de provoquer un empoisonnement. Le terme ciguatera désigne également le phénomène qui en est à l’origine : la destruction des récifs coralliens.
Historique de la ciguatera
La ciguatera est une intoxication connue depuis fort longtemps puisque la première description historique semble être celle d’un médecin chinois de la dynastie des T’ang, Chen Tsang Chi vers l'an 650. À partir du XVe siècle, les progrès de la navigation ont permis aux grands aventuriers de l’époque de partir vers des terres inconnues, où ils ont découvert, à leurs frais, la ciguatera. Ainsi, Colomb, Magellan, Cortes, Vasco de Gama en font la description dans les Caraïbes ; Fernandes de Quiros, Cook, Bligh en font état dans le Pacifique.
James Cook fit la première description précise d'une intoxication à la ciguatoxine, le 7 septembre 1774 aux Nouvelles-Hébrides : « Cet après-midi, un des naturels, ayant harponné un poisson, mon secrétaire l'acheta et me l'envoya après mon retour. Il était d'une nouvelle espèce, un peu comme un poisson-soleil, avec une grosse tête longue et hideuse. Ne nous doutant pas qu'il pouvait nous empoisonner, nous donnâmes l'ordre de l'apprêter pour le souper. Mais par bonheur il fallut si longtemps pour le dessiner et le décrire qu'il n'était plus temps de le faire cuire, de sorte qu'on n'apprêta que le foie et les rognons auxquels monsieur Forster et moi goûtâmes tout juste. Vers trois heures du matin, nous nous trouvâmes atteints d'une extraordinaire faiblesse et d'un engourdissement de tous les membres. J'avais presque perdu le sentiment du toucher et je ne pouvais distinguer, entre ceux que j'avais la force de soulever, les corps lourds des légers. Un quart d'eau et une plume avaient le même poids pour ma main. Nous prîmes tous les deux de l'émétique et après cela nous fîmes une suée qui nous apporta beaucoup de soulagement. Le matin, un des cochons qui avait mangé les entrailles fut trouvé mort. »
Le vocable ciguatera est quant à lui attribué au cubain Felipe Poey, qui l'emploie en 1866 pour désigner une intoxication neuro-digestive consécutive à l’ingestion d’un gastéropode marin (Livona pica) dont le nom vernaculaire cubain est cigua.
Epidémiologie de la ciguatera
La ciguatera concerne environ 400 millions de personnes qui vivent dans les zones d’endémie et on estime à 50.000 le nombre de personnes intoxiquées chaque année. Il s’agit de la plus importante des intoxications par produits de la mer avec l’intoxication histaminique. Cependant, le nombre de cas déclarés est semble-t-il sous-estimé : diagnostic délicat, difficulté d’accès aux soins dans ces régions d’endémie, utilisation de la médecine vernaculaire, difficulté de recueil des informations. La répartition géographique s'étend entre le 35e parallèle nord et le 35e parallèle sud, sur une ceinture circumtropicale englobant l'ensemble des régions coralliennes (Pacifique, Caraïbes et Antilles, océan Indien). Son incidence croît avec la décroissance de la latitude. Plusieurs régions françaises des départements et territoires d’Outre-Mer sont concernées par le phénomène : Réunion (incidence à 7,8/100.000), Guadeloupe (incidence à 30/100.000), Martinique (incidence à 41/100.000), Nouvelle-Calédonie (incidence à 100/100.000), Polynésie (incidence à 500/100.000). La France métropolitaine et les régions situées hors zone d’endémie peuvent également connaître des cas de ciguatera mais ceux-ci sont pour la plupart des cas d’importation contractés en zone corallienne ou liés à la consommation de poissons tropicaux servis en restaurant.
Sous l'effet du réchauffement climatique, de plus en plus de cas sont répertoriés en Europe et notamment en Allemagne où depuis 2012, près de 20 patients atteints de ciguatera sont diagnostiqués chaque année.
Origine de la ciguatera
Le corail est un animal hermatypique, c'est-à-dire bâtisseur de récifs du groupe des madréporaires ou scléractiniaires se présentant sous de multiples formes : encroûtant, massif, colonne, ramifié, foliacé… Les polypes, formant la partie vivante de ces organismes, se logent à l’intérieur des calices calcaires qu’ils élaborent grâce au symbiotisme existant entre eux et de micro-algues photosynthétiques, les zooxanthelles. C’est à l’occasion d’un stress que les polypes se débarrassent de leurs symbiotes, donnant le phénomène de « corail en fleur ». La persistance du stress aboutit à la mort des coraux qui perdent leur source d’énergie ; c’est le phénomène de « blanchissement corallien » (le pigment photosynthétique des zooxanthelles est à l’origine de la couleur du corail).
Le stress à l’origine de cet évènement peut être d’origine naturelle (raz-de-marée, tsunami, tempêtes, cyclones, séismes sous-marins, sources d’eau douce, Acanthaster planci,…) ou d’origine humaine (travaux d’aménagement des littoraux avec utilisation des coraux pour les constructions et formation de nuages de boues privant les zooxanthelles de lumière, pollution des lagons, pêche intensive, tourisme irresponsable, activités militaires…). À grande échelle, le réchauffement climatique à l’origine du réchauffement de la température des mers (le corail souffre à partir de 29° C et meurt au-delà de 30° C) et la surexposition aux rayonnements ultra-violets due aux trous dans la couche d’ozone pourraient également participer à la destruction des récifs.
Ces surfaces coralliennes nouvellement dégradées vont progressivement être recouvertes par des gazons algaux constitués de macro algues sur lesquelles vont à leur tour proliférer des microalgues. Parmi celles-ci, on trouve des algues de la famille des dinoflagellés nommées Gambierdiscus. Dans le Pacifique, six espèces sont décrites : G. toxicus, G.belzeanus, G.australes, G.pacificus, G.polynesiensis, G.Yasumotoi ; seule G. toxicus est à l’origine de la ciguatera. Ses conditions optimales de croissance dépendent de la température de l’eau (entre 26 et 29° C), de la salinité (environ 35 ‰), de la luminosité (de l'ordre de 2.000 à 3.000 lux sur une photopériode de douze heures), du pH (entre 8,2 et 8,4) et de la présence de sels nutritifs (silicates et oxydes telluriques, détritus algaux) et de vitamines (B12, biotine et thiamine). Tout éloignement de ces conditions optimales de croissance entraîne un ralentissement du temps de division. L’intervention de facteurs microbiens dans la croissance des dinoflagellés a également été suggérée par leur rôle d’intermédiaires dans le métabolisme de substances provenant des macro algues ou par l'enrichissement du milieu en dioxyde de carbone (Legrand et al.).
On estime que le délai entre la perturbation du milieu corallien et l'apparition de cas de ciguatera est de l'ordre d'une vingtaine de mois : deux à trois mois pour que les surfaces coralliennes nouvellement mises à nu soit recouvertes de gazons algaux, quatre mois avant que les premiers dinoflagellés soient observés, huit à neuf mois avant que ceux-ci n’atteignent une densité conséquente et encore au moins trois mois pour que soient décrits les premiers cas d'intoxications humaines ; soit, au total, un délai d’un an et demi à deux ans. En l'absence d'entretien du phénomène, l’épidémie dure de dix à trente ans.
La ciguatoxine est un polyéther liposoluble, thermostable, de faible poids moléculaire, considéré comme l’une des plus puissantes biotoxines marines puisqu’il suffit d’à peine un microgramme pour tuer un homme. Les techniques de purification et de détection par chromatographie ont permis d’isoler 39 ciguatoxines différentes. Elles varient selon leur origine géographique, selon les espèces pisciaires et selon leur position dans la chaîne alimentaire. Elles n’ont pas encore toutes livré leur structure moléculaire. La ciguatoxine de référence, la première découverte, la plus représentée et par conséquent la plus étudiée, est la P-CTX1B ; elle sert d’étalon dans les tests de détection en laboratoire. Les ciguatoxines pénètrent la chaîne alimentaire par l’intermédiaire des poissons brouteurs de corail et des herbivores qui broutent les algues sur lesquelles est fixé Gambierdiscus toxicus. Ces poissons sont ensuite les proies des poissons omnivores puis carnivores. Les toxines sont accumulées le long de la chaîne alimentaire, les carnivores présentent donc des taux toxiniques plus importants que les herbivores. De plus, les toxines subissent au sein des organismes pisciaires un métabolisme oxydatif les rendant plus toxiques : les ciguatoxines décelées chez les carnivores sont donc plus nocives que celles retrouvées chez les herbivores. Les CTX étant liposolubles, elles s’accumulent préférentiellement dans certains organes comme le foie, la tête, les gonades ; on en retrouve également dans les chairs mais à des concentrations moindres : l’excès de concentration entre les viscères et le reste des tissus (surtout le muscle) est de l'ordre de 50 à 100 chez Gymnothorax javanicus (murène javanaise). Les toxines ne semblent pas avoir d’effet majeur chez les poissons ; l’accumulation des toxines est un processus lent tout comme le sont les mécanismes de détoxifications hépatiques. Les poissons les plus vieux et les plus gros sont par conséquent ceux qui présentent le plus de risque. Tous les poissons d’ambiance corallienne sont donc potentiellement ciguatoxiques, plus de 400 espèces de poissons responsables ont été décrits, appartenant à des familles et ordres variés (57 familles, onze ordres). Certains semblent cependant exempts de risque comme les poissons pélagiques qui ne chassent qu’en pleine mer : thons, espadons, marlins, mahimahi… ou des poissons vivant en eaux profondes. Des cas isolés ont pourtant été décrits après leur consommation suggérant la possibilité de transmission des toxines par des chaînes alimentaires annexes, non connues. L’homme s’intoxique donc en consommant ces poissons ; la survenue d’une symptomatologie dépendra de la concentration toxinique : 0,1 μg par exemple pour la PCTX1B.
- Destruction de colonies coralliennes. Colonisation de leur squelette par des microalgues.
- Prolifération d'une algue mono-cellulaire toxino-productrice ingérée par les poissons.
- Ces poissons sont ingérés par les poissons carnivores, de plus en plus gros et voraces : accumulation de la toxine.
- Ingestion humaine, fin de chaîne alimentaire.
Répartition géographique de la ciguatera
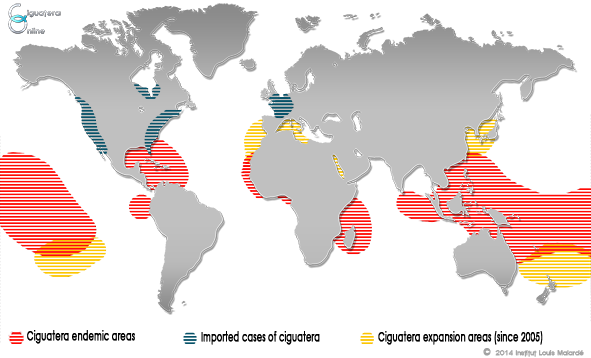
- Il y a risque dans toutes les mers et océans chauds de 20° C et +, entre 30° lat. nord et 30° lat. sud, et d’autant plus que des zones coralliennes sont proches (mais attention, certains poissons font parfois des migrations sur de très longues distances).
- Zones de haute fréquence : voir carte ci-dessus.
- Augmentation globale mondiale régulière semble-t-il.
Tableau clinique de la ciguatera
- Les troubles débutent 1 à 6 heures après l'ingestion du poisson contaminé (extrêmes : 10 min-36 h).
- Le tableau, évolutif, riche et polymorphe, associe diversement trois syndromes et des manifestations générales.
- Syndrome digestif : nausées, vomissements, douleurs abdominales diffuses, diarrhée, le plus souvent aqueuse, parfois responsable de déshydratation aiguë, ténesme, hoquet.
- Syndrome neurologique (95 % des cas) : paresthésies, dysesthésies et confusions froid/chaud, hyperesthésies, arthro-myalgies, douleurs gingivo-dentaires, vertiges, parésies, paralysies.
- Syndrome cérébelleux : une ataxie cérébelleuse peut être observée avec des troubles de la coordination et de l'équilibre.
- Fatigue chronique : asthénie, léthargie, troubles du sommeil avec cauchemars, réveils précoces, intolérance à l'exercice, manque de motivation, douleurs variées, céphalées quotidiennes, etc. Ce syndrome peut être lié aux dysfonctionnements touchant le système nerveux tout entier ou à un état dépressif associé. Sa sévérité n'est pas corrélée à la nature ni à la sévérité de l'intoxication.
- Syndrome dépressif : on ne sait pas si cette dépression est due aux effets de la toxine elle-même ou si elle est secondaire à la phase aiguë de l'intoxication ou au passage à la chronicité de certains symptômes.
- Hallucinations visuelles ou auditives : elles sont notablement plus fréquentes dans l'océan Indien.
- Céphalées, vertiges, étourdissements, ...
- Fonctions cognitives et psychologiques : ne semblent pas être atteintes.
- Syndrome cardio-vasculaire : bradycardie, hypotension artérielle.
- Bradycardie sinusale inférieure à 60 par minute.
- Hypotension artérielle.
- Hypotension orthostatique pouvant persister jusqu'à quatre semaines.
- Beaucoup plus rarement sont observés une hypertension, une tachycardie, un assourdissement des bruits du cœur, des troubles du rythme à type d'extrasystoles ventriculaires ou supraventriculaires, des bradyarythmies, des troubles de la conduction à type de bloc auriculoventriculaire du premier degré. Dans les cas graves, on peut observer un état de choc lié à une défaillance cardio-circulatoire pouvant être majorée par un état de déshydratation aiguë.
- Manifestations générales : hypersalivation ou bouche sèche (précoce), prurit (50 %), sueurs, frilosité, oligurie, déshydratation, asthénie ; érythème (retardé : 2ème jour).
- Myalgies : en particulier les gros groupes musculaires. Deux cas de polymyosite ont même été décrits aux États-Unis chez des patients intoxiqués par la ciguatera quelques années auparavant.
- Arthralgies : elles touchent surtout les grosses articulations, particulièrement les genoux, les chevilles, les épaules et les coudes.
- Prurit : il constitue l’un des maîtres-symptômes de la ciguatera, à tel point qu'il a donné son nom à la maladie en Nouvelle-Calédonie. Ce sont les paumes des mains et plantes des pieds qui sont les plus souvent atteintes. Le prurit peut parfois être généralisé, notamment après l'ingestion d'alcool ou à la suite d'un exercice physique important, c’est-à-dire lorsque le flux sanguin cutané est augmenté. Les démangeaisons peuvent être très sévères et occasionner des lésions de grattage avec leur lot de complications : excoriations, abcès, cellulites, cicatrices, lichenification.
- Éruptions cutanées : lésions éruptives non spécifiques érythémato-papuleuses, avec parfois une desquamation lors de la phase de guérison.
- Frilosité, frissons sans fièvre.
- Hypersudation, hypersalivation, hyperlacrymation, rhinorrhée.
- Raideur de nuque.
- Dysurie, rétention aigüe d'urines.
- Goût métallique dans la bouche, douleurs dentaires, sensation de dents qui se déchaussent, douleurs gingivales.
- Hydrophobie.
- Dyspnée asthmatiforme.
- Flou visuel voire perte de vision transitoire, ophtalmoplégie, diplopie, douleurs rétro-oculaires, injection conjonctivale, photophobie, mydriase ou myosis, ptosis.
- Prurit vulvaire, dyspareunie (certaines femmes dont les symptômes sont chroniques ressentent une recrudescence des troubles au moment de leurs règles).
- Douleurs péniennes lors de l'érection avec intensification au moment de l'éjaculation, pouvant empêcher l'homme d'avoir des relations sexuelles pendant plusieurs semaines. Douleur testiculaire, urétrite avec sensibilité du méat.
- Létalité : selon les études et les pays : 0,1 à 2 %. Ailleurs, guérison spontanée en une à plusieurs semaines.
Diagnostic de la ciguatera
- Il repose sur la notion de consommation récente de poisson en zone inter- ou sub-tropicale.
- Les cas groupés fréquents.
- Le diagnostic est exclusivement clinique, aucun examen paraclinique n’étant disponible à ce jour.
Traitement de la ciguatera
Il n'existe pas d'antidote spécifique : le traitement est purement symptomatique, avec si besoins :
- traitement d'un collapsus cardio-vasculaire, d'un arrêt respiratoire
- réanimation hydroélectrolytique
- atropine en cas de bradycardie
- anti-histaminiques pour le prurit (efficacité inconstante, voire contestée)
- éviter boissons alcoolisées
- vitaminothérapie B ou placebo.
Prévention de la ciguatera
Soit s'abstenir de toute consommation de poisson dans les zones à risque, ou se contenter de manger des petits poissons herbivores ; sinon tenter de diminuer le risque en tenant compte des éléments suivants :
Le risque ciguatérique est augmenté d'autant plus que le poisson est :
- plus gros
- plus âgé
- plus hideux
- plus carnivore
- Quelques poissons sont particulièrement à risque : barracuda, baliste, mérou, mulet, perroquet, poisson chirurgien, requin
- Ne manger de poisson que si formellement identifié comme non ciguatérique par les pêcheurs, restaurateurs ou consommateurs locaux (encore que ces expertises aient été prises en défaut dans de récentes publications)
- Test populaire (non infaillible, non vérifié scientifiquement et peu politiquement correct) : faire ingérer une partie du poisson à un animal domestique (chien, chat, poulet) et attendre d'éventuels symptômes
Dans tous les cas, ne jamais manger les viscères, le foie, la tête des poissons dans les zones à risque.
Enfin, bien noter que cuire le poisson ne diminue en aucun cas le risque, les toxines étant thermostable.